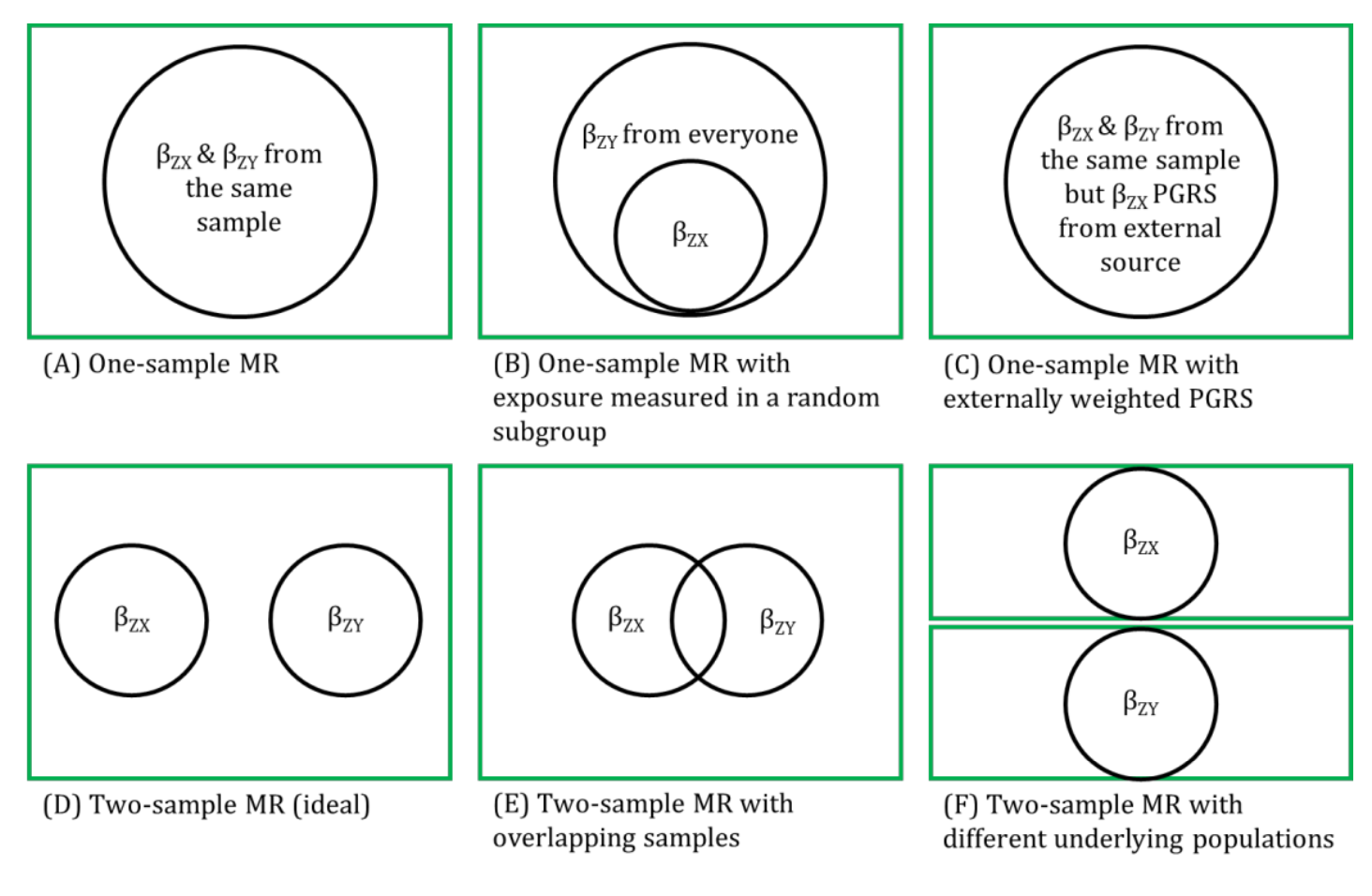
This refers to exaggerated results, whereby there is a bias of estimates away from the null, occurring when MR studies are done within the same sample (e.g., the sample that contributed towards the genome-wide association study (GWAS)) from which the genetic instrumental variables (IVs) are selected.
Ideally, selecting genetic IVs from the same study in which the MR analysis is being conducted should be avoided to reduce this overfitting. Using weighted polygenic risk score (PRS) in one-sample MR where the weights of the genetic IV-exposure association are taken from an independent GWAS minimises bias due to overfitting. Two-sample MR, where genetic IV-outcome associations are obtained from an independent GWAS from the GWAS of the exposure, and there is little or no overlap between the two samples, avoids overfitting.
References
- Zheng J, Baird D, Borges MC, et al. Recent Developments in Mendelian Randomization Studies. Curr Epidemiol Rep 2017; 4: 330-345.
- Lawlor DA, Harbord RM, Sterne JAC, Timpson NJ, Davey Smith G. Mendelian randomization: using genes as instruments for making causal inferences in epidemiology. Statistic in Medicine 2008; 27: 1133-1163.
Other terms in 'Sources of bias and limitations in MR':
- Assortative mating
- Canalization
- Collider
- Collider bias
- Conditional F-statistic for multiple exposures
- Confounding
- Exclusion restriction assumption
- F-statistic
- Harmonization (in two-sample MR)
- Homogeneity Assumption
- Horizontal Pleiotropy
- Independence assumption
- INstrument Strength Independent of Direct Effect (InSIDE) assumption
- Intergenerational (or dynastic) effects
- Monotonicity assumption
- MR for testing critical or sensitive periods
- MR for testing developmental origins
- No effect modification assumption
- NO Measurement Error (NOME) assumption
- Non-linear MR
- Non-overlapping samples (in two-sample MR)
- Pleiotropy
- Population stratification
- R-squared
- Regression dilution bias (attenuation by errors)
- Relevance assumption
- Reverse causality
- Same underlying population (in two-sample MR)
- Statistical power and efficiency
- Vertical pleiotropy
- Weak instrument bias
- Winner's curse